



Sehat Card Scandal: PTI Corruption Allegations, Mismanagement, and Public Loss (2018–2022)
The Sehat Card program, launched with the promise of free, universal health coverage, became one of the Pakistan Tehreek-e-Insaf (PTI) government’s flagship welfare initiatives. Between August 2018 and April 2022, it expanded nationwide, offering each family coverage of up to Rs. 1 million for medical treatment.
However, official audits and investigative reports later revealed deep flaws—mismanagement, weak oversight, and corruption allegations. The heaviest losses were recorded in Khyber Pakhtunkhwa (KP), PTI’s political stronghold, where the Auditor General of Pakistan (AGP) found more than Rs. 28.61 billion in financial irregularities.
(August 2018 – April 2022) — Sehat Card Record and Corruption-Related Concerns
During PTI’s rule from August 2018 to April 2022, there were major issues of fund misuse and suspected corruption in the Sehat Card program. Most irregularities were reported in Khyber Pakhtunkhwa (KP), where PTI was in power. According to the Auditor General of Pakistan (AGP), over Rs. 28.61 billion in financial irregularities were found in the health department, including the Sehat Card scheme. These issues arose from poor management, violations of rules, and possible corruption. Based on official audit reports and credible news sources, here is an easy-to-follow explanation of how this happened.
Corruption Reports and Allegations
1. Excessive Surgeries and C-Sections in Punjab
In Punjab, after PTI expanded the Sehat Sahulat Card program in 2019, significant issues arose, particularly with private hospitals. Total payments for C-Sections under the program reached Rs. 16.36 billion, with nearly 80% of the 525,619 procedures conducted in private hospitals, including Rs. 8.16 billion in 2022 alone. Many of these C-Sections were medically unnecessary, driven by profit motives, which harmed patients and misused taxpayer money. These issues highlight a significant diversion of public funds to private healthcare providers, with weak oversight contributing to corruption and inefficiencies.
Sources: Khyber News, Dawn, The Express Tribune
2. Over-Treatment and Fraud
Some private hospitals exploited the program by performing up to 48 surgeries in a single day, conducting unnecessary C-Sections, and adding extra treatments for multiple patients. One private hospital billed Rs. 900 million for treatment of specific diseases—an amount later ignored by regulators. (Sources: Arab News, Business Recorder, Dawn)
3. Referrals from Public to Private Hospitals
Many public hospitals directly referred patients to private facilities, reportedly in exchange for financial incentives. On average, out of 1,500 patients each month, around 300 were shifted to private hospitals. (Source: The Express Tribune)
4. Investigations and Political Response
In March 2024, Punjab’s finance minister announced an investigation into alleged corruption in the Sehat Card program. (Sources: Arab News, Business Recorder, Dawn)
5. Financial Irregularities in KP
The AGP’s report revealed shocking figures—over Rs. 28.61 billion in financial irregularities in KP’s Sehat Insaf Card program. (Sources: Wikipedia, Facebook, Instagram)
6. Inquiry into Taimur Jhagra
KP Health Minister Taimur Jhagra faced allegations of corruption linked to the Sehat Card program, procurement of medical equipment, and COVID-19 relief funds. (Source: Khyber News)
Global or International Comparison — Similarities and Differences
Internationally, while there have been corruption cases in health insurance or cashless health card systems, no scandal has been documented on the same scale and intensity as in Pakistan.
Universal health coverage and government-funded health insurance face fraud and irregularity risks worldwide:
-
India (Ayushman Bharat PM-JAY): Over 1,100 hospitals removed and 1,500+ fined for fraudulent claims. (Source: Medical Dialogues)
-
Philippines (PhilHealth): 2020–2024 saw major corruption allegations, legislative inquiries, and fake claims controversies. (Sources: Devex, Inquirer.net)
-
Mexico (Seguro Popular, 2003–2019): Billions in irregularities and ghost payments, eventually replaced by INSABI. (Sources: Mexico News Daily, BNamericas)
-
Indonesia (JKN): Research documented billing for unperformed services, unnecessary tests/treatments, and kickbacks. (Source: CMI – Chr. Michelsen Institute)
Fraud risk is a recognized global challenge in government-funded health insurance. Solutions combine data analytics, strict hospital credentialing, biometric/digital auditing, and swift punitive action—gaps that were especially evident in Pakistan.
Program Launch and Expansion
-
Federal Expansion: After starting in KP in 2015, PTI’s federal government expanded the “Sehat Insaf Card” nationwide on February 4, 2019.
-
Punjab Launch: In December 2021, Prime Minister Imran Khan launched the “Sehat Card” program in Punjab, making it available in almost the entire country, offering up to Rs. 1 million per family for treatment.
Administrative Weaknesses and Poor Monitoring
Vacant Key Posts: In Punjab, the Sehat Card team (PHIIMC) had the positions of CEO and COO vacant for two years, with operations running on an ad-hoc basis. This led to inconsistency and susceptibility to influence.
Transparency and Alleged Figures
On social media and in public discussions, allegations were made of around Rs. 10 billion in corruption. However, no conclusive and officially verified government report exists to confirm this—these remain unverified claims.
When monitoring is weak and incentives are misaligned, welfare programs turn into profit-making opportunities. The burden of such misuse eventually falls on citizens in the form of higher taxes, inflation, and public debt.
Impact on the Public
The cost is not only financial but also human:
-
Unnecessary medical procedures (e.g., repeated C-Sections instead of normal deliveries).
-
Use of substandard or harmful medical practices (e.g., Avastin case—contaminated injections causing loss of eyesight in dozens of patients).
Such patterns intensify when private-sector participation is high and public oversight is weak. In KP’s 2021 data, 69% of patients went to private hospitals and 31% to public hospitals, with per-patient costs significantly higher in private facilities. (Source: AGP report)
AGP Findings — Rs. 28 Billion+ Irregularities in KP Health Card
In August 2025, the AGP report revealed that between 2017–18 and 2021–22, the KP Health Card and health sector faced over Rs. 28 billion in irregularities, including payments to 17 unregistered hospitals and weak tax deductions. (Government/department responses are reportedly in process.)
Where the System Failed — Key Cases and Figures
-
Unusual Shift Towards C-Sections in Punjab
Dawn reported that between 2018–2022, a very high share of deliveries under the program were C-Sections—197,376 compared to 97,390 normal deliveries—mostly in private hospitals, raising concerns of financial incentives driving unnecessary surgeries. -
Fraudulent/Incorrect Claims and Unnecessary Admissions
The Express Tribune (2023) documented tactics such as fake admissions, unnecessary surgeries, and inflated billing—the more the claims, the higher the payments.
Breakdown of Key Irregularities
| Problem | Details | Amount Involved | Example |
|---|---|---|---|
| Payments to unregistered hospitals | Hospitals not approved by Health Care Commission still received payments, violating the State Life Insurance agreement. | Over Rs. 2 billion for two hospitals | Anwar Hospital & Kings International Hospital in Swat got Rs. 1.028 billion each without registration. |
| No tax deduction | Govt paid State Life without deducting 8% income tax. | Rs. 2.16 billion loss | Full payment made without tax cuts from 2017–2022. |
| Extra hiring without need | Overstaffing in 32 district hospitals without justification. | Rs. 824 million | Wasted on excess cleaning/security staff. |
| Breaking procurement rules | Contracts awarded without open tendering, violating KP’s KPPRA rules. | Rs. 198 million | One company received all contracts without competition. |
| Advance payment without work | Funds given for hospital repairs, but work never started. | Rs. 1.072 billion | Paid to Punjab’s Infrastructure Development Authority; no progress by April 2023. |
| Overcharging by private hospitals | Private hospitals treated fewer patients but charged far more. | Rs. 882.7 million in one case | Sardar Khan Private Hospital (14,999 patients) vs. Bacha Khan Complex (29,911 patients at Rs. 338.2 million). |
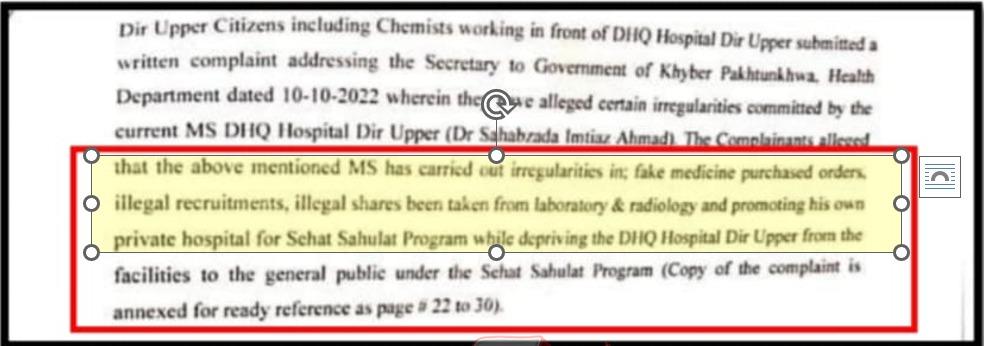
Major Irregularities Exposed in Sehat Insaf Card Program: The Ikhlas Medical Center Case in Upper Dir
The Sehat Insaf Card (Sehat Sahulat Program), designed to provide free healthcare to low-income families in Khyber Pakhtunkhwa, continues to face serious questions over systemic corruption and misuse. A suppressed inquiry report has brought to light a disturbing pattern of irregularities at Ikhlas Medical Center, a small private hospital in Upper Dir district.
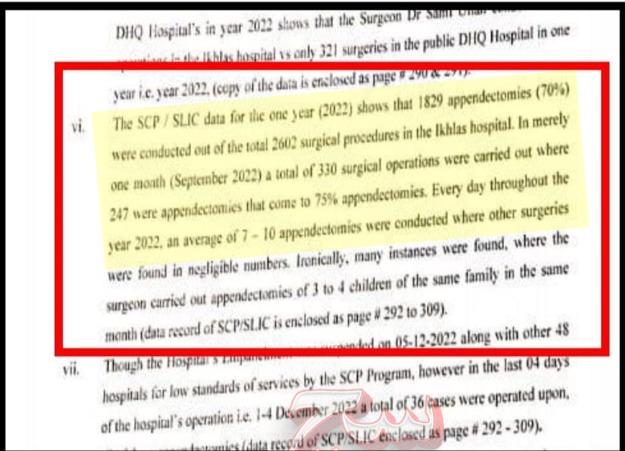
In a single year under review, the facility performed a total of 2,602 surgeries, of which an extraordinary 1,829 (approximately 70%) were appendectomies (appendix removals). Even more alarming, around 75% of these procedures were concentrated in just one month — a statistical anomaly that strongly suggests potential over-treatment or fabricated claims rather than genuine medical need.
Central to the case is Dr. Samiullah, a surgeon employed at the government’s District Headquarters (DHQ) Hospital in Upper Dir and a co-owner of Ikhlas Medical Center (alongside Dr. Sahibzada Imtiaz Ahmed). During the same period, Dr. Samiullah personally conducted 773 operations at the private facility — more than double the 321 surgeries he performed at the public DHQ Hospital in the entire year. This stark disparity raises serious concerns about conflict of interest: the public hospital appears to have been used as a referral pipeline or “launchpad” to funnel Sehat Card patients toward the private setup for financial gain.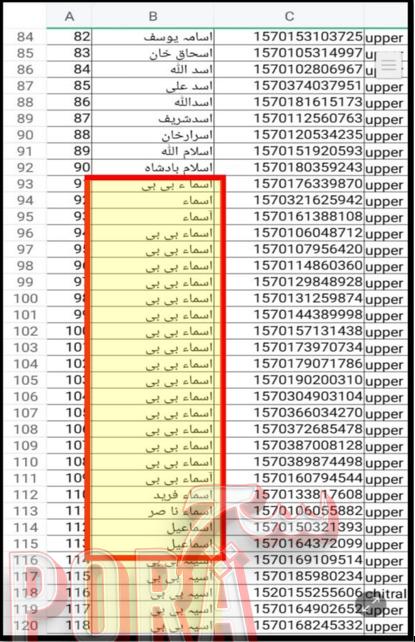
Notably, Ikhlas Medical Center was not actively empanelled or recognized under the Sehat Card scheme at the time, yet numerous procedures were reportedly billed through the program. As a result, Dr. Samiullah alone received over Rs 30 million (3 crore rupees) in reimbursements from the insurance provider, primarily for appendix-related claims.
This episode marked one of the first formal provincial-level inquiries into the Sehat Card program. The committee recommended immediate clinical audits of all Sehat Card-funded surgeries to verify medical necessity and detect fraud. It also called for expanded investigations across other districts and private hospitals to assess the full extent of irregularities.
The Ikhlas Medical Center scandal highlights deeper structural vulnerabilities in the program: inadequate monitoring, weak oversight of private facilities, conflicts of interest among public-sector doctors, and the risk of exploiting a welfare scheme meant for the vulnerable. Without rigorous reforms — including real-time verification, mandatory third-party audits, and strict penalties for misuse — such incidents will continue to erode public trust and divert scarce resources away from genuine patients who need them most.
This case serves as a stark reminder that while initiatives like Sehat Insaf Card hold immense potential to transform healthcare access, their success depends entirely on transparent governance and zero tolerance for corruption.
The Ikhlas Medical Center Scandal – A Window into Potential Systemic Abuse in Khyber Pakhtunkhwa’s Sehat Insaf Card Program
Location: Upper Dir District (Deer Bala area), Khyber Pakhtunkhwa, Pakistan Facility Involved: Ikhlas Medical Center (a small private hospital jointly owned by Dr. Sahibzada Imtiaz Ahmed and Dr. Samiullah, a surgeon also employed at the government District Headquarters (DHQ) Hospital) Period Under Scrutiny: Primarily data from 2022 (one-year review period referenced in reports) Key Allegations: Massive over-performance of surgeries — especially appendectomies — billed under the Sehat Insaf Card program, raising questions of fraud, conflict of interest, and misuse of public welfare funds.
An inquiry committee formed by the Khyber Pakhtunkhwa Health Department uncovered alarming irregularities at Ikhlas Medical Center, a private facility in a remote district with a population of approximately 1.1 million. The hospital reportedly performed 2,602 surgeries in a single year under the Sehat Insaf Card scheme — an extraordinary volume for a small private setup.
Of these, 1,826 (over 70%) were appendectomies (appendix removals). Dr. Samiullah, a co-owner and practicing surgeon at both the private hospital and the government DHQ Hospital, personally conducted 773 of these appendectomies at Ikhlas Medical Center. In the same period, he performed only 321 surgeries at the public facility — highlighting a clear disparity that suggests the government hospital may have served as a referral mechanism or “launching pad” to channel Sehat Card patients to the private hospital for financial benefit.
The facility was not actively empanelled under the Sehat Card program at the time, yet claims were processed through the insurance mechanism. Data from the insurer revealed payments exceeding Rs 30 million (primarily for appendectomies) to Dr. Samiullah alone, accounting for about 70% of the hospital’s total claimed reimbursements.
The inquiry flagged several red flags indicative of potential fraud:
- Extreme concentration: Up to 10 appendectomies per day in some periods, resulting in appendectomies comprising over 70% of all surgeries at the hospital — far exceeding global benchmarks (where appendectomies typically represent ~1.2% of surgical cases).
- Unusual family patterns: Multiple family members (sometimes two or more from the same household) undergoing appendectomies, which is medically improbable without strong epidemiological justification.
- Suppression of the report: The two-member committee’s findings were reportedly suppressed during the previous PTI-led government, delaying accountability.
The committee’s recommendations included:
- Immediate clinical audits of Sehat Card-funded surgeries province-wide.
- Physical verification (e.g., examining surgical scars) among affected families to confirm whether procedures were genuinely performed or if identities were misused for claims.
- Expanded probes into other districts and private hospitals to determine if similar patterns exist.
This case is considered one of the first formal provincial inquiries into the Sehat Insaf Card program and has fueled calls for nationwide scrutiny, with some observers describing it as potentially emblematic of one of Pakistan’s largest healthcare-related scandals.
Hospital Response (for balance): The administration of Ikhlas Medical Center has defended the figures, noting that the district’s population supports an average of about 150 appendectomies per month (or ~5 per day) across the year. They emphasize that their facility offers a range of services (hernia repair, cholecystectomy, C-sections, URS for kidney stones, tonsillectomy, etc.), but appendectomies dominate due to high referral volumes for urgent procedures. They argue that the per-1,000 population rate remains below national/international averages and is not anomalous given local healthcare access gaps.
Broader Implications: The Ikhlas Medical Center case exposes vulnerabilities in the program’s design: weak monitoring of private providers, conflicts of interest for public-sector doctors with private stakes, inadequate verification of medical necessity, and risks of over-billing that divert funds from genuine beneficiaries. Subsequent developments — including restrictions on private hospitals performing certain procedures (e.g., appendectomies) under the program and larger audits revealing billions in irregularities — underscore the need for reforms like real-time claim validation, third-party audits, and stricter empanelment criteria to protect this critical welfare initiative.
This standalone case can be inserted as a separate subsection in your article (e.g., under a heading like “Spotlight Case: Ikhlas Medical Center – Evidence of Potential Fraud”). It maintains factual integrity, adds analytical weight (e.g., explaining statistical anomalies and systemic risks), and presents a balanced view.
Authentic Reference Links:
Document 1: Append
Document 2: Ikhlas-Medical-Center-Upper-Dir-Data
Document 3: inquiry-report-1
Frustrations with Sehat Insaf Card Implementation
Some people claimed Sehat Card holders are humiliated or treated as second-class — with upfront cash payers getting priority and faster service, while card users face long delays (e.g., months-long waits), raising questions about real accessibility and fairness in the program’s implementation at private facilities.
Trigger: A posted a video that went viral on social media (widely shared, including on Twitter/X by accounts like @SydTauqeerShah).
Location: Fatima Memorial Hospital, Lahore, Pakistan Date: Around mid-February 2022
In the footage, a man is seen holding his Sehat Insaf Card (Qaumi Sehat Card) at the hospital’s OPD, visibly angry and frustrated. He claimed he was unable to access free treatment for his son’s hernia condition despite having the card.
Main Complaint (as voiced in the video):
- His son was suffering from hernia, experiencing severe pain and difficulties in daily activities (e.g., sleeping and sitting properly).
- He approached Fatima Memorial Hospital seeking a hernia operation.
- Hospital staff reportedly told him:
- Immediate treatment/surgery was available only if paid upfront in cash.
- If using the Sehat Card for the operation, he would have to wait 2 months.
The man continued recording his interaction in the OPD until hospital staff and police intervened and stopped him.
Consequences — Rising National Debt
Poor economic policies or corruption (like the Sehat Sahulat Card issues) can worsen the debt burden, as public funds are misused instead of being used productively. International lenders may impose strict conditions (e.g., IMF reforms), which can lead to austerity measures, affecting the public through higher costs or fewer services.
Rising debt can lead to inflation, higher prices, and a weaker rupee, reducing people’s purchasing power. For example, the exchange rate jumped from Rs. 105 per dollar in 2017 to around Rs. 200 by 2022, making imports (like fuel and food) more expensive for everyone.
In short, the debt is ultimately paid by Pakistani citizens through taxes, reduced services, and economic pressures, with the burden potentially lasting for decades if not managed well. If you want more details or a specific aspect explained, let me know!
Question
Who Pays the Debt?
Answer : You & Your Future Generation
One major outcome was the increase in Pakistan’s per capita debt:
-
2017: $1,027 (~Rs. 108,000) per person.
-
April 2022 (June 2022 data): $1,277 (~Rs. 216,709 to Rs. 256,000) per person.













{kind=link}